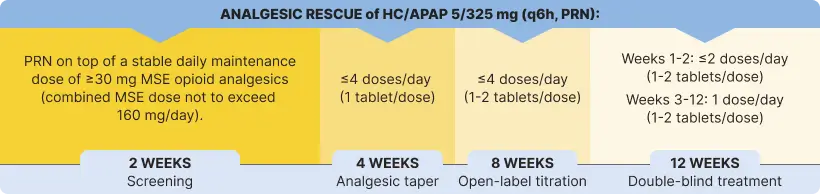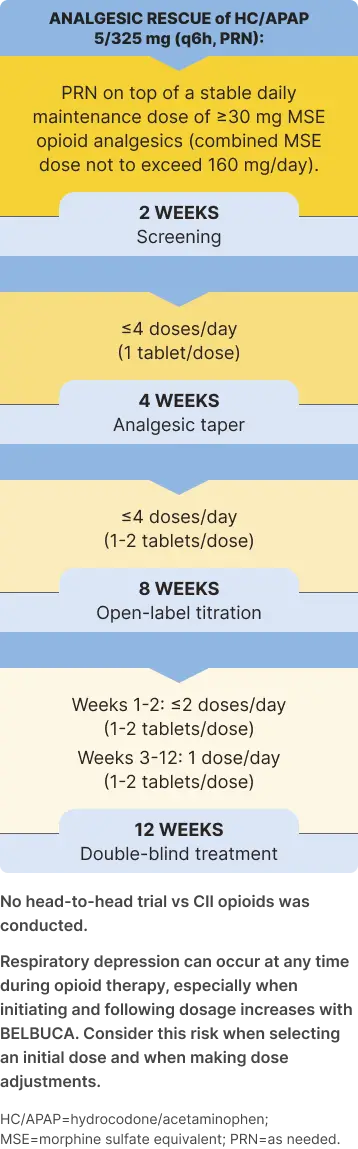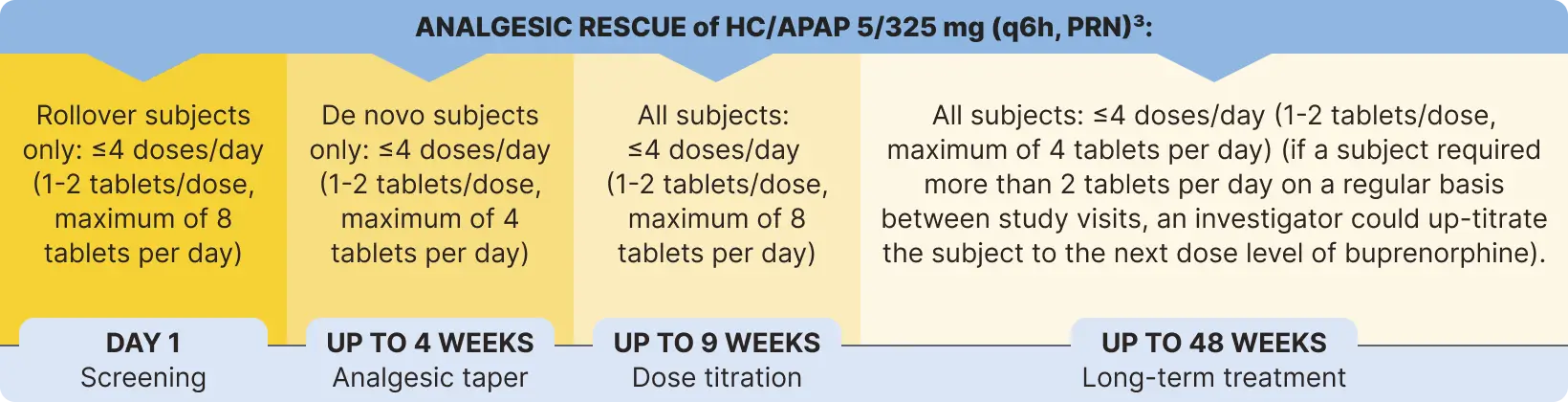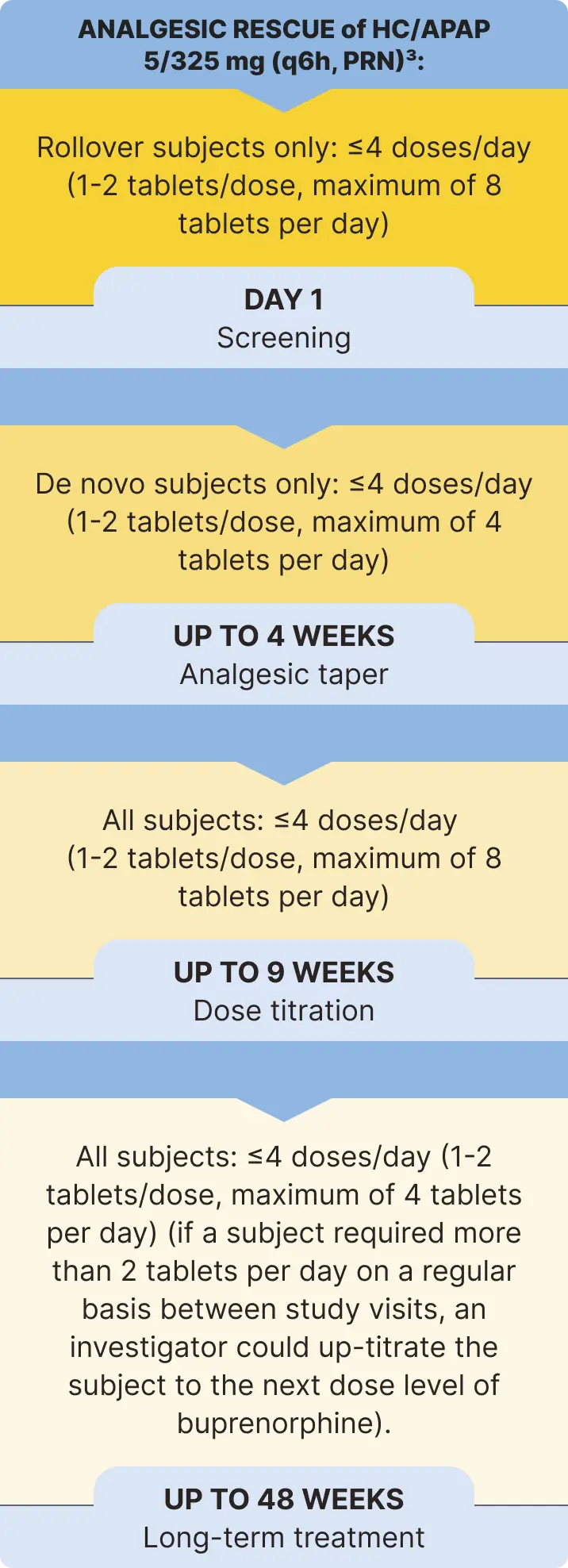
Screening: Opioid-experienced patients with moderate to severe chronic pain3
of patients reported poorly controlled pain on their current opioid medications at screening (of the patients randomized to the double-blind treatment phase)4,5
Opioid medications used in ≥5% of patients: hydrocodone (57%), tramadol (34%), oxycodone (19%), and morphine (5%).5*
*No head-to-head studies vs CII opioids or short-acting opioids were conducted.
Inclusion criteria3
- Opioid-experienced patients (30- to 160-mg/d MME) with moderate to severe chronic low back pain taking around-the-clock opioid analgesics
- Back pain was non-neuropathic (classes 1 and 2), neuropathic (classes 3-6), or symptomatic for 6 months after low back surgery (class 9) at the time of screening